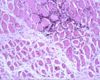
Atrophic muscle fibres (Image sourced from Bristol Biomed Image Archive with permission) - Decreased myofibre or whole muscle diameter
- Myofibrils removed by disintegration -> sacrolemma too large -> forms folds
- Caused by:
- Disuse atrophy (e.g. fracture, failure to use limb, recumbency)
- Slower than denervation atrophy
- Reversible unless too prolonger or severe to cause loss of myofibres
- Pressure atrophy
- Any prolonged pressure on muscles resulting in muscle atrophy
- Abscesses, neoplasms, parasitic cysts
- Denervation atrophy
- Any interference or damage to its nerve supply results in muscle atrophy
- Can be rapid - over 50% of muscle mass may be lost in a few weeks e.g. roarer horses with laryngeal hemiplegia
- May be reversible if innervation re-established
- Histologically:
- Fibres become rounded in cross section unless compressed by normal fibres
- Increased concentration of nuclei as they take much longer to disintegrate
- Fibrous stroma of epimysium and endomysium condenses -> more prominent
- End result in muscle consisting of almost only fibrous tissue
- Sometimes replaced by fat tissue -> increased size of muscle = pseudohypertrophy
- Muscle may have a mixture of atrophied and hypertrophied (due to increased work load) fibres if some motor units are not damaged
- Nutritional atrophy for nutrients during:
- Malnutrition, cachexia, senility
- Gradual onset except for some febrile diseases causing cachexia
- Postural muscles are not affected, sometimes even hypertrophy
- Histologically:
- Some nuclei disappear as myofibre volume is decreased
- Grossly:
- Smaller, darker, thinner muscles
- Senile atrophy
- Similar to nutritional atrophy.
- Lipofuscin pigmentation is common
- Grossly:
- Yellow-brown / dark brown colour (esp in diaphragm)
