Maxillofacial Trauma
Introduction
Imaging and Diagnosis

Lateral and DV skull radiographs together with intra-oral dental radiographs facilitate the diagnosis of maxillofacial injuries. Lateral and DV skull radiographs alone result in too much bony superimposition of structures. Dental radiographs are also higher definition images showing subtle changes.
CT scans demonstrated 2.0 times more maxillofacial injuries in cats compared with conventional radiographs. The average number of maxillofacial injuries per animal by radiographs and CT-scan was 3.8 and 7.7 in cats, respectively. CT allows for accurate assessment, diagnosis and treatment planning of maxillofacial trauma in cats however is not always available at the time of injury or may not be possible due to financial constraints. '
Treatment
The treatment goals are:
- Realignment to normal occlusion
- Minimal invasiveness
- Minimal morbidity
- Early return to self-feeding
- Pain control
When dealing with facial fractures, the repair has to be stable but not necessarily rigid. The use of intramedullary pins, plates, and screws is cautioned against as it can easily result in tooth root damage. Pins, plates, and screws have further disadvantages: they are expensive and require specialized equipment and training. The upper jaw and the nasal cavity consist of thin bone plates that are very difficult to fix rigidly. Intraosseous wire fixation is limited but surgical techniques using special mini-plates have proven useful and enable good realignment of fractures.
Specific Injuries
Maxillary and Temporomandibular Joint Injury
Maxillary fractures are often more subtle to diagnose compared with mandibular fractures and may provide reasonable healing with conservative management only (pain management and soft food).
Signs of maxillary trauma can include:
- Malocclusion of particular teeth or an entire arcade
- Traumatic oronasal communication
- Epistaxis
- Swelling of the maxillary or nasal region
Patients suffering documented maxillary injuries should also be evaluated for changes in ocular position and movement as this is indicative of traumatic injury involving the extra-ocular muscles or insertion locations on the orbital rim.

Malocclusion due to maxillary trauma

Midline Palatal Separation
Midline palatal separation is seen primarily in cats that have fallen from a height or been involved in a road traffic accident (RTA).
Treatment consisting of suturing the mucosa is usually adequate for relatively stable bone fractures. Debride wound edges and place simple interrupted sutures. Rarely do these need advanced flap techniques to close the separation. Use monofilament absorbable suture material (not PDS as this is too stiff).

Midline palatal separation

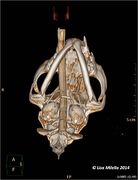
Radiograph of midline palatal separation


Palatine Fractures
Unstable fragments from maxillary and palatine shelf fractures result in a malocclusion due to a shifting of the maxillary arcade. Osteosynthesis using cerclage wire and/or a transfixation pin or reconstruction of the dental arch using locking bone plate and screw systems is recommended. Intra-oral splints made from acrylic can be used to stabilize fractures if the displacement is not too severe.

Palatine fracture

Incisive Bone Fractures
These fractures are usually minimally displaced and can be repaired using cerclage wire and acrylic splint quite successfully.

Incisive bone fracture

Zygomatic Arch Fractures
These are often associated with trauma to the eye and orbit. The fracture can result in displacement of the eye caudally or ventrally if the lateral support is lost or can result in exophthalmos if the bone fragments are displaced medially.
Conservative management of the fracture is usually recommended. If internal fixation is necessary, extreme caution should be exercised to avoid damage to the facial nerve or maxillary artery (in caudal fractures).
Zygomatic arch fracture

Temporomandibular Joint Fractures
These are usually seen in combination with other maxillofacial injuries. Depending on the degree of displacement, the fracture may or may not result in a malocclusion. The fracture may involve the condylar process (of the mandible) and/or the mandibular fossa of the temporal bone of the maxilla.
If the articular surface of the joint is involved, then a condylectomy is recommended. If not, maxillomandibular fixation is usually adequate. In some cases a muzzle may suffice. Restoration of the alignment of the maxillary and mandibular canine teeth and application of maxillomandibular fixation in a partial open mouth position is reasonably well accepted by most patients. Use of repair techniques such as this provides the benefits of a less invasive repair technique, no disruption of the fracture hematoma, and reduced risk of damaging the blood supply to nearby teeth.

Condylar process fracture

Mandibular fossa fracture

Maxillomandibular fixation

Maxillomandibular fixation




Further Reading
- The Diagnostic Yield of Conventional Radiographs and Computed Tomography in Dogs and Cats with Maxillofacial Trauma, Bar-am et al Y, Veterinary Surgery, Volume 37, Issue 3, pages 294–299, April 2008
- Dental Composite for the Fixation of Mandibular Fractures and Luxations in 11 Cats and 6 Dogs, Bennet J et al, Veterinary Surgery, Volume 23, issue 3, pages 190-194, May 1994
- Horner's syndrome associated with a mandibular symphyseal fracture and bilateral temporomandibular luxation, Baines S, Journal of Small Animal Practice, Vol 42, issue 12, pages 607-610, Dec 2001
- Verstraete FJ & Lommer M, ed, Oral and Maxillofacial Surgery in Dogs and Cats. Edinburgh, UK : Saunders Elsevier, 2012, p363-372
| This article was written by Lisa Milella BVSc DipEVDC MRCVS. Date reviewed: 22 October 2014 |
| Endorsed by WALTHAM®, a leading authority in companion animal nutrition and wellbeing for over 50 years and the science institute for Mars Petcare. |
Error in widget FBRecommend: unable to write file /var/www/wikivet.net/extensions/Widgets/compiled_templates/wrt6a2945c155cf39_21331533 Error in widget google+: unable to write file /var/www/wikivet.net/extensions/Widgets/compiled_templates/wrt6a2945c15bbaf3_29078078 Error in widget TwitterTweet: unable to write file /var/www/wikivet.net/extensions/Widgets/compiled_templates/wrt6a2945c16091f5_89725576
|
| WikiVet® Introduction - Help WikiVet - Report a Problem |